"Veterinary Specialist Services Pty Ltd.")
Case Study: Portosystemic Shunt
Kimba, a female Bichon Frise crossbreed was only three months old and 2.8kg when she showed blood in her urine and frequent attempts to urinate, with only small amounts of urine produced. She was also lethargic and much smaller than her litter mate. Her regular vet performed a biochemistry profile which showed ALT: 244 slight elevation 2-3 x normal, and ALP: 580 slight elevation 2-3 x normal. A urine sample was taken, which showed ammonium biurate crystals. She was placed on a course of oral amoxycillin/clavulanate suspension, and the haematuria resolved.
Pre and post-prandial bile acid tests were performed, which showed elevated fasting bile acid (468 umol/L) (normal range 0-11) and elevated post-prandial (230 umol/L) (normal range 0-21). High bile acid concentrations indicate reduced hepatic function or altered bile and/or blood flow, including that associated with portosystemic shunting. Based on this information, a portosystemic shunt was expected, and she was referred to Veterinary Specialist Services (VSS) for further assessment and treatment.
On presentation at VSS, Kimba was quiet and alert and no neurological signs were seen - other than her being a bit more subdued than expected for a puppy and about half the size of her litter mate. A bladder ultrasound found two large stones in her bladder. Her haematuria had resolved, but she was still urinating small amounts at a time and wanting to go to the toilet frequently. She was put on a low protein diet and an oral metronidazole and oral lactulose solution for four weeks prior to her CT scan; and during this time, she gained 1kg. A CT scan was scheduled for further diagnostic evaluation of the presence and type of portosystemic shunt. Levetiracetam was started 48 hours prior to her anaesthesia for her CT scan.
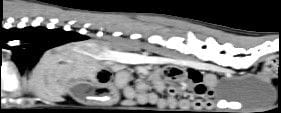
The CT showed a single extrahepatic LEFT gastrocaval portosystemic shunt, a small liver and two large calculi in the urinary bladder.

Transverse post-contrast images of the abdomen in soft tissue window and 3D reconstruction of the portal vasculature.
She recovered well from anaesthesia - although she did need to be placed on a glucose drip until she was eating well on her own. She was sent home the same day and cellophane banding of the shunt was scheduled for the following week.
At surgery, the shunt was located in the left aspect of the prehepatic caudal vena cava just caudally to the liver. The shunting vessel was short, wide and thin walled. A cellophane banding technique was used to partially occlude the shunt.
 on the left and cellophane banding on the right.")
Gastrocaval PSS (blue arrow) on the left and cellophane banding on the right.
Kimba also had two large uroliths removed via a small cranioventral cystotomy. They can be seen here on the pre-operative CT scan - and i/v contrast can be seen in the PSS and the caudal vena cava.
Kimba recovered well post-operatively with supportive care in ICU for 24 hours and then the hospital ward for a further four days. She showed no deterioration in her neurological signs after surgery and was discharged four days after surgery with ongoing amoxyclav, metronidazole, lactulose, a low protein diet and oral probiotic powder.
At her ten-day recheck, she was doing well with no change/deterioration in her neurological signs. The wound had healed well, and her sutures were removed. She had gained 300g since surgery and was urinating normally.
Her bile acids levels will be monitored again eight weeks after surgery to evaluate liver function. We will maintain a protein-restricted diet for a minimum of eight weeks post-op, and after blood test values return to normal, approximately three months after surgery, if tolerated, the diet will be progressively returned to normal. Lactulose and oral antibiotics will continue for approximately eight weeks (metronidazole). Lactulose will be stopped a few weeks later, if there are no signs of hepatic encephalopathy. The liver will begin to grow as the shunt closes and will often return to normal size and function in two to four months.
The prognosis is excellent for animals that survive the immediate post-operative period and where full ligation of the shunt is achieved. With partial ligation, the prognosis is not as good. In many cases, full ligation is possible in animals that were partially ligated 4-6 months previously; so, follow-up bile acids tests will help guide ongoing treatment.
In general, surgery is recommended for PSS, but medical management is possible. Surgery is associated with an 80-90% long-term good outcome, with some dogs requiring ongoing medical management. Perioperative complication rates are in the 6-12% range and can be life threatening. Medical management is associated with a good medium-term outcome in 33% of cases, however the overall average survival time is 9-10 months.
| Tags:GastrointestinalHaematologyVSS Resource Area |