"Veterinary Specialist Services Pty Ltd.")
Analgesia for the Surgical Patients
Analgesia for the Surgical Patient
Anita Parkin RVN, AVN, Dip (Surgery & ECC), VTS (Anesthesia /Analgesia), CVPP, TAE Veterinary Specialist Services Pty Ltd, Brisbane, Queensland, Australia
Pain Pathway
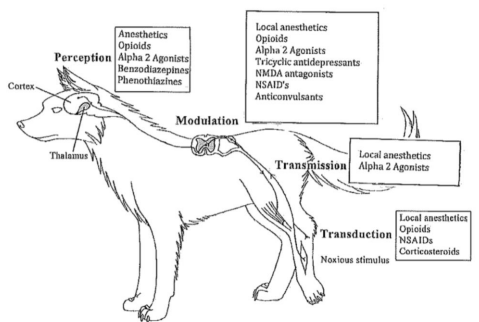
Figure 1: Pain Pathway and the Classes of Drugs that Work on each part of the Pain Pathway
Nociception – is the sensory process that provides the signals up the pain pathway leading to the ability to feel pain
Noxious Stimulus – stimulation of the nerve ending
Transduction – transmits the noxious stimulus into a nerve impulse that can then travel
Transmission –transmits the nerve impulse to the spinal cord
Modulation – Spinal cord amplification (or suppression) of a pain signal, before it gets to the brain
Perception – This is not considered as part of the nociceptive process, but it is a result of successful transduction, transmission and modulation of the noxious stimulus
Types of Analgesics
Types of Analgesics: Historically, the most common classes of agents used for analgesia were opioids and NSAID’s, however, it is now becoming more common to add in different classes of drugs (local anesthetics, NMDA antagonists, and alpha 2 agonists) to form a multimodal approach to give our patients overall better pain relief. The class and type of drug that you choose for your patients will depend on the patient’s signalment, perfusion status, temperature, route of administration, pharmacokinetics and the pharmacodynamics of the particular drug that you are considering to administer.
All opioids have a similar mode of action, though the receptors that they are active on can vary. Different receptor types include: OP1 (), OP2 (), and OP3 (). Most agonist drugs work on the receptors, which are considered superior analgesics, and are the drugs of choice used for moderate to severe pain relief.
Agonist
Agonist: Pure or full opioid agonists can elicit maximal activation of the receptor when they bind to it, and the subsequent downstream processes produce a maximal analgesic effect.
Morphine: Morphine is a full agonist opioid that works on receptors. It is a natural narcotic with a duration of action of 3 – 4 hours. Morphine should be used with caution IV due to the histamine release and also from stimulation of mast cell degranulation. Morphine can be administered IM, SC, IV, PO and via the epidural space (preservative-free). Due to its poor lipid solubility administration via the epidural space means that it will last 12 – 24 hours.
Fentanyl: Fentanyl is a pure agonist, with 100x potency compared to morphine. It has a fast onset of action (5 minutes), and short duration of action (30 minutes) making it ideal to run as an IV continuous rate of infusion (CRI). Main side effects, when used in high doses, are apnea and bradycardia, so ventilation should be closely monitored.
Fentanyl is highly lipid-soluble, so is ideal for transdermal infusion (patches) at a dose of 2 - 4mcg/kg. After application of the patch, it takes approximately 24 hours (dogs) and 12 hours (cats) to reach peak effects and lasts up to 72 hours post-application.
Methadone: Methadone is a synthetic pure agonist that is 1.5 – 4x the potency of morphine. Duration of action is 2 – 4 hours, can be given IV, IM or SC in dogs (0.1 – 0.5mg/kg) and cats (0.1 – 0.3mg/kg) and oral transmucousal (OTM) in cats (0.6mg/kg). Patients are less likely to vomit on methadone compared to morphine, however it can cause more dysphoria in patients than morphine. Methadone also possesses additional affinity for NMDA receptors and alpha 2 adrenergic receptors.
Oxymorphone: Oxymorphone a synthetic pure opioid that is 10x the potency compared to morphine. It is less likely to cause patients to vomit after administration and will provide more sedation than morphine. It is good to use in patients that are respiratory compromised (brachycephalic breeds), as it is less likely to cause panting. Duration of action is 4 – 6 hours.
Hydromorphone: Hydromorphone is a synthetic pure opioid that is 5 -10x the potency compared to morphine. It has similar properties to oxymorphone, but is more expensive than oxymorphone. Injections can be given IV, IM or SC to dogs and cats (0.05 – 0.1mg/kg) duration of effect is 4 – 7 hours.
Meperidine: Meperidine is a synthetic pure opioid that is 1/8 the potency of morphine. If given IV it should be given slowly due to its histamine release and hypotensive effects. Dose rate for dogs and cats is 3 – 5mg/kg IM, SC and duration of action is 1 – 2 hours.
Remifentanil: Remifentanil is a derivative of fentanyl that is short-acting (6 minutes in dogs and 17 minutes in cats), and is approximately 50x potency compared to morphine. This drug is unique as it is metabolized by non-specific plasma esterases to inactive metabolites, independent of hepatic/renal metabolism. Therefore, it is good for the use in patients with liver/renal dysfunction.
Agonist-Antagonist
Agonists-antagonists: are competitive receptor antagonists, but will still have analgesic effects by stimulating other receptors (k). They are good to use for mild pain, but cannot be effectively used in conjunction with pure agonist drugs. These drugs provide good sedation qualities.
Butorphanol: Butorphanol is an agonist-antagonist drug that provides good sedation when used in conjunction with acepromazine or benzodiazepines. Butorphanol works at the receptors that have shown to be 5x the potency compared to morphine at these receptors and will antagonize drugs at the receptors. Duration of action is 1 – 3 hours and can be administered IV, SC, IM. Butorphanol has also been shown to have antitussive qualities, making it good to use in patients with dyspnea caused by a collapsing trachea.
Partial Agonists
Partial agonists: are drugs that bind to receptors but only produce a limited clinical effect. Increasing the doses will not increase the amount of analgesia as they have a ceiling effect – it will only last a longer duration. They are useful for mild to moderate analgesia.
Buprenorphine: Buprenorphine is a semi-synthetic partial agonist, with little to no effect at receptors. It has a very high affinity for receptors (and can displace morphine from these receptors) but cannot elicit a maximal clinical response; therefore, it is used to treat mild to moderate pain. Duration of action is between 6 – 12 hours depending on the dose and route of administration. Buprenorphine can be administered IV, SC and IM for dogs and cats (0.005 – 0.02mg/kg) and cats can also be given via the OTM / buccal mucusally (0.04 – 0.12mg/kg).
Antagonists
Antagonist: drugs have high affinities for the opioid receptors at the and receptors. Antagonists will bind to these receptors and will rapidly reverse all opioid-induced clinical effects – including analgesia.
Naloxone: Naloxone duration of action is short (30 – 60 minutes) and will reverse all opioid agonist effects, producing increased alertness, responsiveness, coordination and increased perception of pain. Due to its quick onset of action (1 – 2 minutes IV) naloxone should be titrated to effect (0.002 – 0.02mg/kg) to avoid adverse effects of excitement and anxiety. Premature ventricular contractions may be seen but are not common. Due to the short duration of action, it may be necessary to provide additional doses as the patient may become narcotized as this drug becomes inactive. Naloxone can be used to reverse pure agonist and agonist-antagonist, but the greater affinity to the receptors does not reverse buprenorphine as well.
Non-Steroidal Anti-Inflammatory Drugs (NSAID’s)
NSAID’s: are drugs that have antipyretic, anti-inflammatory and analgesic properties. Most NSAID’s are administered per os, but some are also available in injections (meloxicam). NSAID’s are generally metabolized in the liver and may have active metabolites.
NSAID’s are effective analgesics and of significant benefit for all types of pain and intensities. NSAID’s can be administered in the perioperative period (meloxicam), as well as different types of acute and chronic pain states. For chronic pain states, it should be used as part of a multi-modal approach to provide efficient analgesia
NSAID’s are contraindicated in patients with hepatic disease, gastrointestinal (GI) ulceration, patients that are having vomiting or diarrhea, dehydrated, hypotension, heart failure and patients that have renal insufficiency.
Local Anaesthetics
Local anaesthetics: are drugs that reversibly bind to the Na+ channels and block impulse conduction in nerve impulses. Sensations disappear in the order of pain, cold, warmth, touch, deep pressure and return in the opposite order. Sensory blockade will usually persist long that motor blockade. Lidocaine can be safely administered IV, but Bupivacaine is cardiotoxic, so should not be administered via this route. Lidocaine dosing for dogs is up to 6mg/kg (cats 3mg/kg) for a duration of action of 1 – 2 hours. Bupivacaine dosing for dogs is up to 2 mg/kg (cats 1mg/kg) for a duration of action of 2 – 6 hours. Both of these drugs can be used in conjunction with opioids to increase the duration of action and to provide a good multi-modal approach to analgesia.
NMDA Antagonists
NMDA antagonists: (ketamine) at very low doses can contribute to a good multi-modal approach to analgesia. It adds analgesic effects by minimizing CNS sensitization, however, they are not considered ’standalone’ analgesic agents. For surgery patients: ketamine should be started prior to surgery and continued 24 hours post-surgery. This has been shown to increase appetite and produce lower pain scores, for trauma cases, it should be initiated as soon as possible. Dogs have a loading dose of 0.5mg/kg followed by a CRI at 0.2 - 2mg/kg/hr.
Alpha2 Adrenergic Agonists
Alpha2 adrenergic agonist: is used to produce sedation and hypnosis, analgesia and muscle relaxation. The analgesic effects are short-lived in comparison to the sedative effects. They are reversible and are metabolized in the liver (excreted via the kidneys).
Side effects of these drugs include hyper and/or hypotension, bradycardia, hypothermia, decreased sympathetic tone and GI motility, increase in urine output, emesis, salivation and bradyarrhythmias. They should not be used in patients with cardiopulmonary disease, pre-existing hypo/hypertension, diabetes mellitus and liver/renal failure. The use of anticholinergics in combination with alpha2 may be contraindicated if peripheral vasoconstriction and possible hypertension are present.
Alpha2 can be used in conjunction with opioids and inhalant anesthetics and generally the doses can be reduced when alpha2 is used.
Monitoring of patients
Monitoring of patients: For patients that are being treated for acute pain it is recommended they be assessed every 15 – 30 minutes post-surgery and then hourly for 6 – 8 hours then every 3 – 6 hours thereafter. Using pain scales will assist you in determining if your patient will require more analgesic drugs or less.
For patients that are being treated for chronic pain, they too should be assessed on a regular basis. Getting the owners to fill out a pain scale report (questions) or asking questions to see the progress of the patient is generally required to see if the drug protocol is effective for that patient, or not. This should be followed up closely before dispensing more drugs and further blood tests may be required for ongoing medication.
| Tags:MedicationVSS Resource Area |